The subject of Covid-19 deaths is a sensitive one. Losing a loved one to illness is a painful experience, and raising questions about the validity of the official cause of death is understandably seen as callous or uncaring. More aggravating are those individuals who really do behave in a callous or uncaring manner when they hear about a Covid-19 death. When someone is openly grieving on social media, for instance, about having lost a friend or relative to Covid-19, it is not uncommon for someone to leave a truly unsympathetic comment such as, “Was it really a Covid death, or were there underlying conditions?”
Such a person may well be aware of some of the things I will be sharing here, but that awareness does not excuse the total lack of empathy and kindness that civil society rightly demands at such a moment. There is a proper time, place, and manner for sharing information, and it pains me to see grief magnified and educational opportunities lost through such discourteous attitudes.
Unfortunately, inaccurate, inflated reports on Covid-19 death numbers have circulated from the very beginning, and this must be addressed.
In April 2020, the “Worldometer,” a tracking site that publishes and updates data from the WHO and the CDC, showed that the U.S. was reporting 12 deaths per million people. This was very typical; most countries were reporting similar or much lower numbers:
From April 2, 2020:
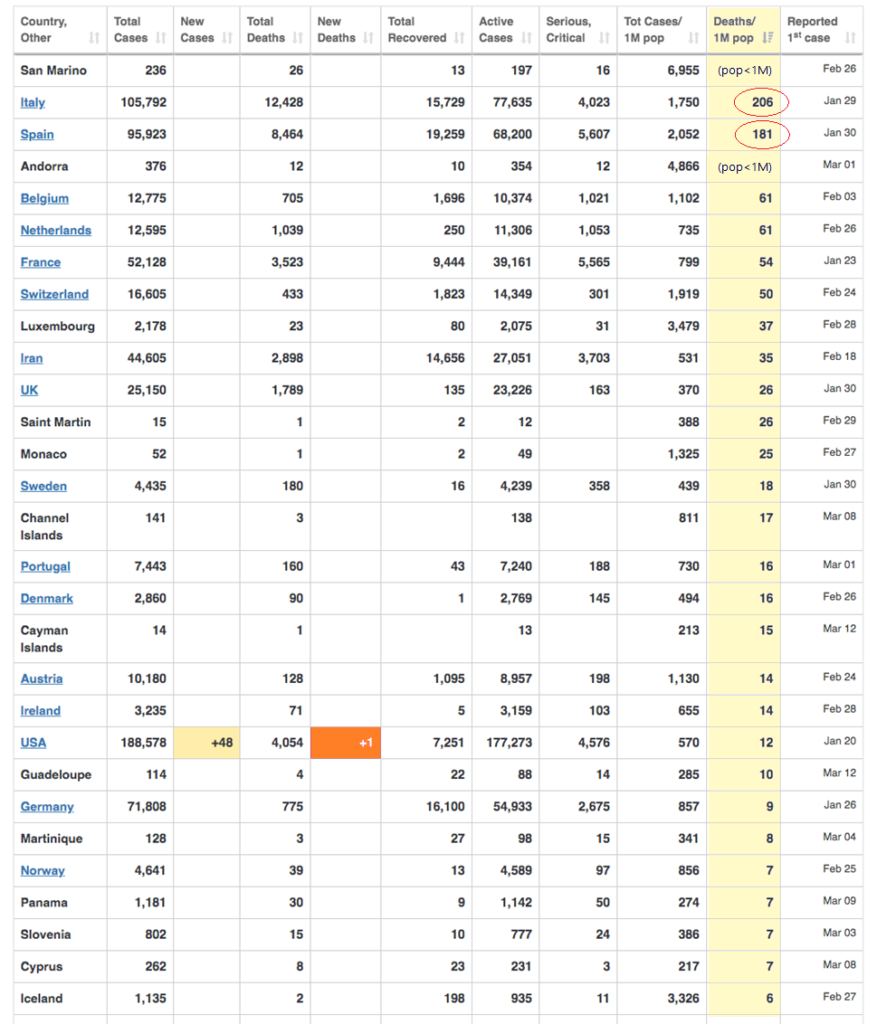
In fact, of the 180+ nations reporting Covid-19 deaths, there were only two with death rates that might have been of worldwide concern: Spain and Italy. The obvious question should have been, “What’s going on in Spain and Italy?” Unfortunately, almost every news outlet simply sensationalized Italy’s death toll, highlighting but rarely questioning the very atypical death rates.
A careful look at this Telegraph article from March 2020 quickly clears up the mystery of Italy’s unusually high Covid-19 numbers. Buried amongst largely unsatisfactory explanations about the average age of Italy’s population and their overburdened hospital staff is this particularly valuable nugget:
“Italy’s death rate may also appear high because of how doctors record fatalities.”
How doctors record fatalities? Professor Walter Ricciardi, scientific advisor to Italy’s Minister of Health, elaborates, as reported in that same article and elsewhere:
“The way in which we code deaths in our country is very generous in the sense that all the people who die in hospitals with the coronavirus are deemed to be dying of the coronavirus. On re-evaluation by the National Institute of Health, only 12 per cent of death certificates have shown a direct causality from coronavirus…”
While most of us understand that a viral illness can exacerbate an existing health problem and turn a bad condition into a fatal one, we also realize that this is not new to Covid-19. What is new is hearing the scientific advisor explain that Italy is using a different method to code their deaths than other countries are using – a “generous” method, as he put it – and we should note that important distinction as we react to the numbers, so we can put them into context.
Professor Ricciardi was not the only one who attempted to clarify the unusual way that Italian deaths were being classified. At a briefing on March 20, 2020, Angelo Borrelli, the head of Italy’s Civil Protection Service, also made a point of distinguishing between dying with this coronavirus and dying because of it, cautioning, “I want you to remember these people died WITH the coronavirus and not FROM the coronavirus.” (If you’re fortunate enough to speak Italian, you can listen to his words here at the 3:30 mark.)
Taking Professor Ricciardi at his word that only 12% of recorded Covid-19 deaths were directly attributable to Covid-19 illness would bring Italy’s April 2020 death rates completely in line with those of the rest of the world. These rates are similar to death rates from the flu in past years – nothing that would warrant global travel restrictions, lockdowns, business closures, the masking of healthy people, or isolating our sick and elderly, leaving them to languish among strangers.
Unfortunately, caveats from people like Professor Ricciardi and Angelo Borrelli were not heeded, and these destructive policies were launched globally, all because of the fear fomented by these artificially high death tallies.
What about now? A look at the Worldometer today will show that many countries are currently reporting death rates far higher than would be expected during typical or even very bad flu years. Are these numbers accurate?
Not even close.
Part of the inaccuracy is explained on the CDC website:
“As of April 14, 2020, CDC case counts and death counts include both confirmed and probable cases and deaths.”
If you have read about how “probable cases” are determined, you will likely be dismayed to learn that the same broad, subjective criteria are used to determine “probable deaths.” No Covid-19-specific test is required, and no symptoms are necessary for a diagnosis (or even posthumous diagnosis) of Covid-19.
As reported U.S. death numbers began to climb to alarming levels, former CDC director and White House Coronavirus Response Coordinator Deborah Birx explained that the U.S. had also adopted “liberal” counting methods, in which anyone dying with Covid-19 would be counted as dying from Covid-19:
CDC guidelines were taken to extremes all over the country. Here are just a few examples:
Los Angeles
As explained in this L. A. Times article, “Los Angeles County public health officials said their tally of COVID-19 deaths includes any person who died from a heart attack, stroke or another ailment if they had tested positive for the coronavirus within the last 90 days.”
Oregon
According to this NBC news article, Oregon Health Authority spokesman Jonathan Modie explained that “[d]eaths in which a patient hospitalized for any reason within 14 days of a positive COVID-19 test result dies in the hospital or within the 60 days following discharge” are counted as Covid-19 deaths. Regarding a hypothetical case of someone who had tested positive for Covid-19 and then died in a motorcycle crash, Modie was asked whether that would be counted as a Covid-19 death. “It would be,” he said.
Arizona
As reported in this ABC news article, in Maricopa County, Arizona, county health department official (and CDC field officer) Rebecca Sunenshine explained, “Even if it’s not listed on their death certificate, anyone who has a COVID-19 positive test within a certain period of when they died, is also counted as a COVID-19 positive death.”
Another spokesperson specified, “Someone who was diagnosed with COVID-19 by a PCR test and died within 60 days of their diagnosis would be considered a COVID-associated death.”
Colorado
This news report highlights fraudulent classification of Colorado deaths that were clearly due to other causes as Covid-19 fatalities, including a man who died of alcohol poisoning and whose blood alcohol level was .55% – seven times the legal limit and well beyond what is considered a fatal concentration:
Additionally, according to the report, LaPlata county coroner Jann Smith listed “congestive heart failure” as the cause of death for one man, “but the local health department then listed the 80-year-old’s death as ‘LaPlata County’s first Covid death’…”
New York
Even more shocking, in April 2020, New York City actually reclassified thousands of previous deaths as Covid-19 weeks or even months after the deaths occurred and absent any testing or evidence of Covid-19 infection.
Not only did these extra 3,778 “probable” deaths appear as a spike in New York fatalities, but they raised the national total by 17%. Again, the supposedly increasing death toll was widely publicized, while reports of the shenanigans behind the increase were relatively sparse and often couched within articles claiming that fatalities were being underreported.
This NBC article quotes Dr. Oxiris Barbot, commissioner of the NYC Health Department, who actually lamented that people who had died of heart attacks (with no coronavirus symptoms) should have been counted as Covid-19 deaths:
“Some deaths, for example, could have been registered as having been caused by heart attacks because people had not yet developed coronavirus symptoms, when they should have been counted as probable COVID-19 victims.”
The bottom line: fatality rates have been greatly exaggerated from the very beginning and throughout the alleged Covid-19 crisis, leading people all over the world to accept a slew of unprecedented policy measures that have proven physically, mentally, and economically devastating.
____________________
Extras:
Interview with Erin Olszewski – Nurse Erin Olszewski shares her experience at Elmhurst hospital in New York City and exposes the tragic consequences of Medicare’s financial incentives in diagnosing and treating Covid-19. (70 min.)
For a shorter synopsis of the interview, click here. (11 min.)