“If it saves just one life…” is a common justification for a host of uncomfortable, unnatural, and, as we have seen, unnecessary behaviors that include requiring perfectly healthy adults and even little children to mask their faces; avoiding the elderly; withholding visits to grandparents; isolating from friends, coworkers, and classmates; restricting travel; destroying the livelihoods of millions; postponing life-extending medical procedures to make room for a hypothetical influx of Covid-19 patients; furloughing doctors and nurses when that influx doesn’t happen; preventing loved ones from comforting sick or dying family members; and even forbidding grieving families from mourning together. Trying to imagine how any of this – let alone all of it taken together – could possibly be in our best interest as individuals or as a society requires some extraordinary mental gymnastics.
Yet many of us perform those intellectual contortions, twisting what we have always known was good and appropriate into something dangerous, selfish, or uncaring. It’s selfish to breathe fresh air in public without a mask. It’s dangerous to visit Grandma and Grandpa. It’s uncaring to want to hold Dad’s hand as he prepares for surgery.
What if none of that is actually true? What if black is not white? What if down is not up? What if good is not evil?
What if, by trying to protect one person, we destroy another? Or many others?
The cruel policies, senseless suffering, and many, many preventable deaths from neglect, abuse, and suicide are by far the most painful and inexcusable aspects of these demonstrably unwarranted restrictions. Certainly now, after a full year of this, we should be stepping back to honestly evaluate the damage, no matter how painful it is.
Suicides
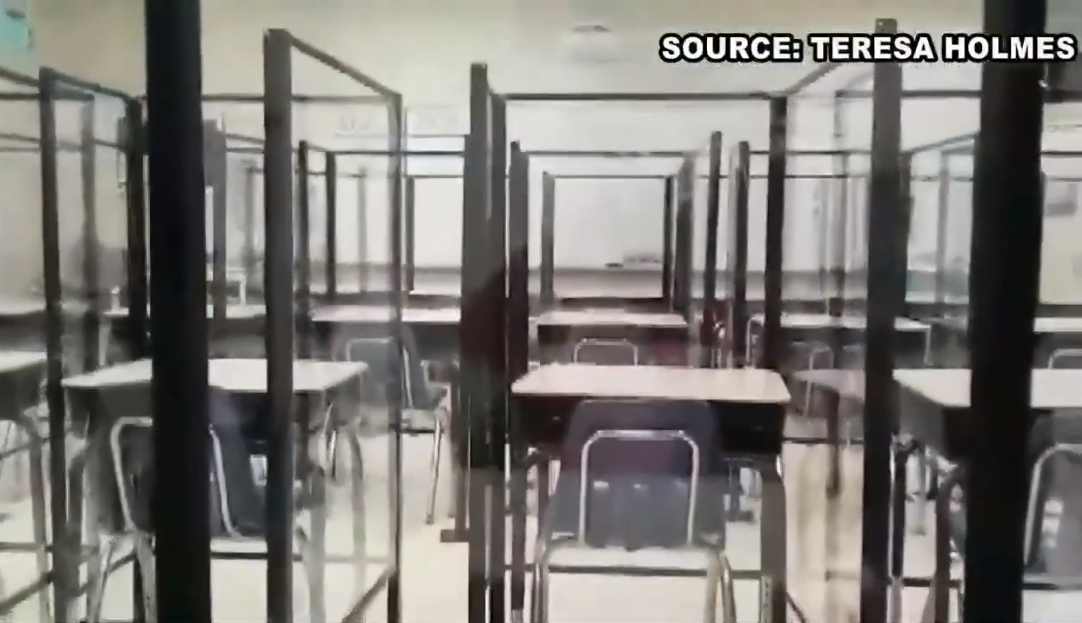
This now prison-like elementary school classroom in Horry County, South Carolina, is just one of thousands all over the country installing Plexiglas barriers. Here is a small sampling of similar news reports from schools in Alabama, Colorado, Georgia, North Carolina, Texas, Utah – even South Africa – and more barriers are being constructed every day. According to the chair of the Horry County Board of Education, these unnatural and unprecedented attempts to keep children from spreading germs cost $5 million.
But if it saves just one life…
But what if it doesn’t? What if children have a far lower risk of even becoming seriously ill with Covid-19, let alone dying from it? And what if feelings of depression and disconnectedness put the children at far greater risk of dying by suicide than from the virus?
While the total number of deaths involving Covid-19 for ages 0-17 from the beginning of the pandemic through March 20, 2021, is 238 (updated March 29, 2021), teen suicides – which were already the second leading cause of death among teenagers – number in the thousands every year and increased sharply during 2020. Every death is heartbreaking, no matter the cause, which makes it all the more urgent that we oppose measures that tend to increase feelings of depression, anxiety, and isolation in our children. One Nevada school district of about 300,000 kids had double the number of suicides in 2020 as it had in 2019. That’s nine excess deaths from a single school district. (For what it’s worth, there are approximately 15,000 school districts in the United States.)
In Pima County, Arizona, according to the Foundation for Economic Education:
“…suicides were up 67 percent in 2020 compared to the previous year for children ages 12 to 17, and statewide childhood suicides had also increased since 2019. West Virginia has seen a spike in student suicide attempts during the pandemic. Parts of Wisconsin reported skyrocketing [nearly doubled] suicide rates among young people in 2020, while hospitals in Texas and North Carolina are seeing more young suicidal patients.”
Children and teens are at the lowest risk of anyone for catching Covid-19 and at even lower risk of dying from it. Isolating them, disrupting their lives, and hiding their smiling faces has taken a terrible toll both in terms of young lives and mental health. It is medically irrational and morally inexcusable.
Failure to Thrive
Drugs.com addresses this syndrome as it occurs in the elderly, saying, “Failure to thrive (FTT) happens when an older adult has a loss of appetite, eats and drinks less than usual, loses weight, and is less active than normal. He or she may not be interested in other people or social activities.”
How much more tragic when the decrease in activity and socialization is actually imposed on our elderly, either by government mandate, such as in care centers, or by their own family members who put more trust in official recommendations than in their own compassionate intuition and basic common sense.
As a society, we continue to comply with measures that are not only illogical but medically unsound. Caregivers familiar with it can tell you what “failure to thrive” does to the elderly:
“Geriatric failure to thrive is a syndrome that is causing the deaths of countless senior citizens… Elderly signs of decline are important to take notice of, and failure to thrive in dementia patients is especially important to watch out for….
“The individual with failure to thrive syndrome is failing to live. They’re slowly dying.” Listed among telltale symptoms are decreased appetite; inactivity; persistent feelings of sadness; a “lack of interest in activities the individual would normally enjoy”; and, importantly, impaired immune function.
Normally, people intuitively know that the most helpful remedies for this kind of decline include visits, hugs, shared meals, group activities, and outings – and that withholding those things from our seniors actually contributes to their decline. Now, however, institutions and individuals have placed caution above compassion, to the detriment of our elderly loved ones.
As Vivian Rivera Zayas, co-founder of Voices for Seniors, pointedly put it, “They are protecting them to death.”
“But with Covid-19, things are different now.”
Things are different now…but should they be? If you have not read about the fraudulent methods for testing, counting cases, and even counting deaths, I hope you’ll do so immediately. Our fear of spreading death and disease is actually contributing to death and disease, and we owe it to our aging parents to thoroughly inform ourselves before complying with damaging and counterintuitive recommendations.
Dying Alone
Despite our best efforts, we will lose loved ones – sometimes even tragically. Even though it is heartbreaking, death is a normal part of the human experience. What isn’t normal is dying alone without the comfort of loved ones during those last moments.
Stories like this one are extremely common:
“The first time Stacey [Silva] tried to visit her dad at the hospital…[h]er father already was isolated behind a solid wood door, and she couldn’t even see his face.” Two weeks later, she watched behind glass doors as he passed away. “’Not being able to talk to my dad, not being able to be by his side was heart wrenching,’ she said. ‘I couldn’t hold his hand when he took his last breath… I feel like he was alone.’”
This New York Times article, “‘A Heart-Wrenching Thing’: Hospital Bans on Visits Devastate Families,” reminds us that there are tangible health benefits to having family members comfort and advocate for their loved ones:
“Clinicians and hospital staff said keeping families away had been among the darkest experience of their professional lives. The restrictions run contrary to a hospital’s desire to keep patients and families together, not only for the salutary [health-promoting] effect of something as simple as a hand held, or a chair pulled close to a bed, but because having a relative present can ease the workload of a medical team. It can also provide crucial information that a confused patient may not be able to offer.”
One 89-year-old Utah man broke his hip and was taken to the hospital, where his children were not allowed to accompany him. They explained to nurses that he had mid-stage dementia and would be disoriented and confused by himself. Still, staff denied entry and promised to call them if there was a problem. Coming out of the anesthesia after his hip surgery, he was confused and upset, as his children had predicted, and reacting poorly to medication. Staff eventually authorized only one of his children to stay in the room with him. Days later, when she became exhausted, they finally allowed one other sibling to alternate with her. Their father continued to decline, however, and it appeared he might not recover. At this point, permission was given for only two of his seven children to be in the room with him. His situation became dire, at which point his elderly wife was at last given permission to visit. Tragically, while she raced to the hospital, he passed away. They had been married for 65 years.
There are thousands, if not millions, of similarly heartbreaking stories.
Another casualty of the harsh restrictions was a younger but obese man in precarious health, who contracted Covid-19. A couple years earlier, he had come down with severe respiratory illness that threatened his life. However, doctors were able to treat him, and he had returned to his normal activities. Now, in early 2020, he again came down with severe illness, testing positive for Covid-19. This time, however, he had been convinced by an irresponsible media that he would almost certainly die, and he knew if he checked himself into the hospital, no family members would be allowed with him. Not wishing to die alone, he chose to stay at home, untreated, and passed away in his bed.
Communicable disease is not new. Even during the worst years of illness, hospitals have successfully relied on preventative measures such as hand-washing stations and asking symptomatic people to refrain from visiting, in order to minimize transmission. There is no justification for governments to dictate hospital policy, and hospitals would do well to give more weight to past experience and sound medical practice than skewed media reports that have little basis in fact. At the very least, they should consider the case-by-case benefits of visits instead of issuing blanket bans.
The bottom line: by trying to avoid causing hypothetical harm, we’re doing actual damage and destroying countless lives.
____________________
Extras:
Dr. Pam Popper discusses an elderly care center patient who opted for assisted suicide over another lockdown.
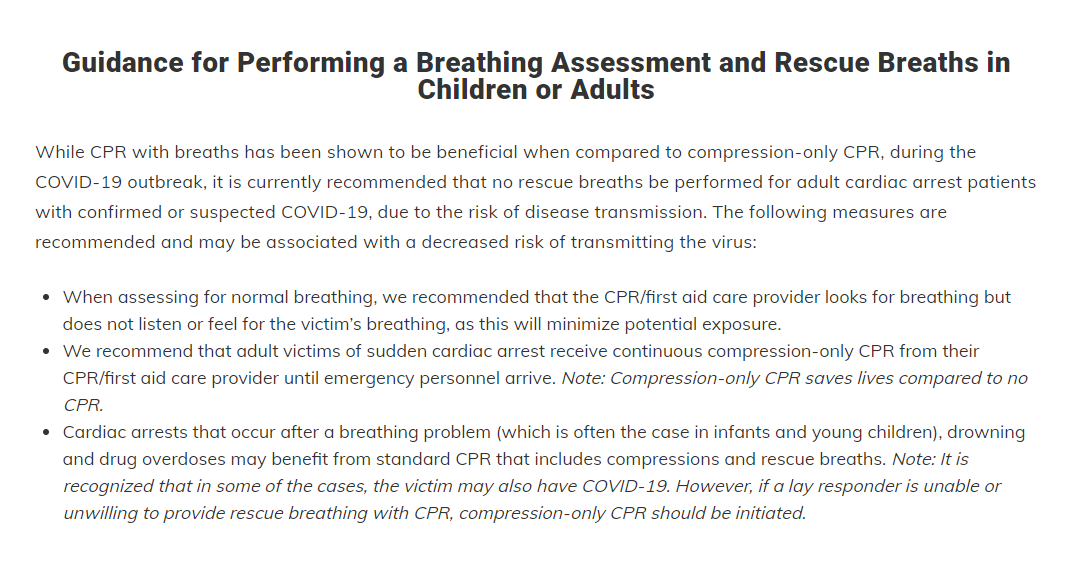
CPR during Covid-19 – As unbelievable as this may be, the Red Cross website literally says, “While CPR with breaths has been shown to be beneficial when compared to compression-only CPR, during the COVID-19 outbreak, it is currently recommended that no rescue breaths be performed for adult cardiac arrest patients with confirmed or suspected COVID-19, due to the risk of disease transmission”:
Returning Canadians quarantined in “designated government facilities” – In January 2021, Canada’s prime minister Justin Trudeau announced that the government was cancelling all flights to Mexico and the Caribbean and would be implementing “other measures” as well:
“In addition to the pre-boarding test we already require, as soon as possible in the coming weeks, we will be introducing mandatory PCR testing at the airport for people returning to Canada. Travelers will then have to wait for up to three days at an approved hotel for their test results, at their own expense, which is expected to be more than $2,000. Those with negative test results will then be able to quarantine at home under significantly increased surveillance and enforcement. Those with positive tests will be immediately required to quarantine in designated government facilities…”
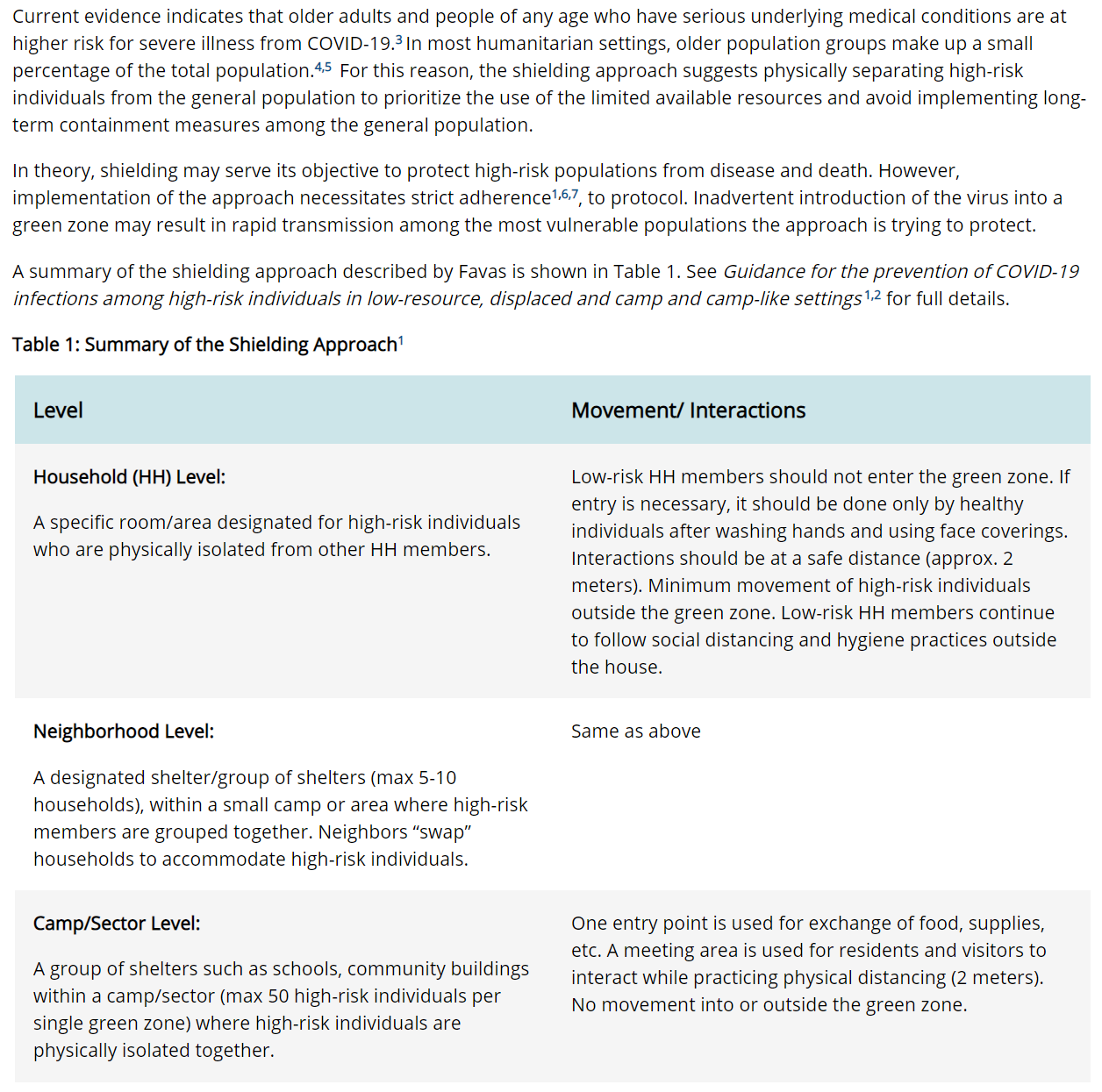
CDC Shielding “Camps” – Plans are in place for potential implementation of “the shielding approach [which] suggests physically separating high-risk individuals from the general population.” (High-risk is loosely defined as “older adults and people of any age who have serious underlying medical conditions.”) This can be done at the neighborhood level, with neighbors trading houses in order to create “green zones” for high-risk groups, or, for a larger “camp,” a school might be used. “One entry point is used for exchange of food, supplies, etc.” and there is “[n]o movement into or outside the green zone.”
From the CDC website: